Dementia Praecox and Paraphrenia
Terminal States and Disease Progression
Chapter 7 of 12 · Pages 169–202
Terminal States and Disease Progression
on account of developing arthritis. A patient sat bent forwards in such a way that her nose dipped in the soup; another held the left thumb always extended, the right bent inwards; a third sat with the mouth open, the tongue stuck in a corner of the mouth. Many patients assume a fencing attitude; a patient continually held his hands as if he wanted to box. Sometimes contractures are developed in the joints that are continually bent; an example of this is given in Fig. 27, which represents a patient who for long years had held his arms pressed against his body and his fingers bent.
In stupor the eyes are either closed, as in the patient represented in Fig. 28; if anything comes near they are tightly closed and the eyeballs rolled upwards, or they are wide open, staring with dilated pupils into the distance, never fixing anything; blepharoplegia takes place extremely seldom. The forehead is drawn up, frequently wrinkled; the expression of the face, vacant, immobile, like a mask, astonished, is sometimes reminiscent of the rigid smile of the akinetans. Figs. 29 and 30 represent the face of the same youthful patient at different stages of a severe catatonic stupor. In the former the face shows more a dazed, rigid perplexity, in the latter that sleepy vacancy which is generally connected, as also here, with catalepsy.
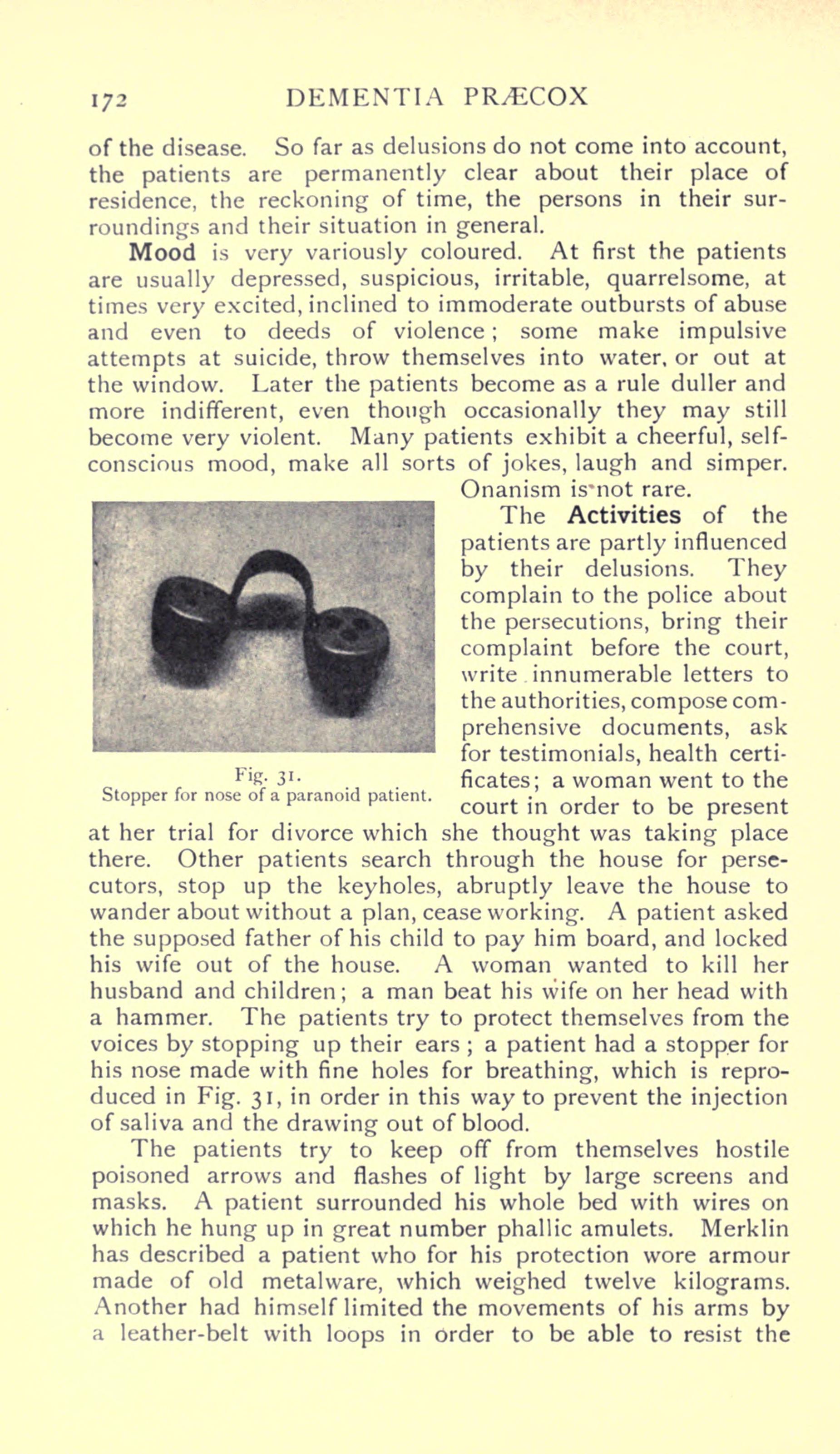
Fig. 30. Expression of face in catatonic stupor (d).
The lips are often pursed forward like a snout (“Snout-cramp”), and show now and then lightning or rhythmic twitchings. Grinning, sudden laughter, and making faces are frequent.
Constraint is also noticeable in the gait of the patients. Often indeed it is quite impossible to succeed in experiments in walking. The patients simply let themselves fall down stiffly, as soon as one tries to place them on their feet. In other cases they march with extended knees, on tiptoe, on the outer edge of the foot, with legs wide apart, with the upper part of the body well bent backwards, sliding, frisking about, balancing, in short, in any wholly unusual attitude which, however, is preserved with all the strength at their command in spite of every external influence. A patient walked with his face turned backwards; a female patient kept accurately to a seam in the floor and did not let herself be pushed to the side. Single movements are stiff, slow, forced, as if a certain resistance had to be overcome, or they are done jerkily and then often as quick as lightning.
The states of catatonic excitement and of stupor, which are here described, and which are apparently so opposed, are obviously very clearly related to each other clinically, as they not only can pass directly the one into the other but are also intermingled in the most varied way. The patient who has just been senselessly excited may suddenly become mute and now lie motionless; the patient who has been stuporous, perhaps for weeks, abruptly begins to utter unintelligible screams at the top of his voice, to call out cock-a-doodle-doo, to bark, to sing a song in a refined voice. Or he leaps with long bounds through the room, as quick as lightning unhinges somewhere or other a window, gives a neighbour a box on the ear, and dashes with tremendous force into another patient’s bed, and then remains again inaccessible or possibly even passes through a longer period of excitement. Such a change of state occurs with fair frequency in our patients. Very often both excitement and stupor last only a few days or weeks, perhaps only a few hours, and then gradually or suddenly disappear. But on the other hand also a uniform clinical state may continue for months, years, and even decades, and be only quite temporarily interrupted by remissions or by some other kind of morbid phenomena. Especially in stupor that happens not very rarely, while catatonic excitement stretching similarly over years belongs, one may say, to the exceptional cases.
The character of the phenomena is in different cases very varied. Stupor may sometimes only be indicated by taciturn, repellent drowsy conduct, rising in other cases to the suppression of volitional discharge, while excitement may fluctuate from slight, silly merriment to the most regardless fury seriously endangering life. We may well regard it as a mixture of the phenomena of both states when a patient dances about mute and with closed eyes, or lies motionless and bawls a street song. Indeed, one may perhaps on the whole connect the negativistic admixtures in the states of excitement, the inaccessibility and the insusceptibility to influence, the resistance, the speaking past a subject, further the indications of automatic obedience, with the admixture of stuporous morbid symptoms. On the other hand we observe in stuporous patients frequently enough single impulsive actions which are otherwise peculiar to the states of excitement. The patients suddenly throw a cup across the room, jump up in order to smash a pane of glass, to go round the table, to throw themselves then head foremost again into bed and lie there motionless, or they give utterance to meaningless sounds or scream, hurrah! The stereotyped movements, which are occasionally observed in stupor, fiddling, pulling faces, spitting, might also be regarded from the point of view of a mixture with the phenomena of excitement. From that, however, not much is gained. Essentially it only appears that we everywhere meet the same fundamental disorders in the different forms of dementia praecox and so also in the catatonic forms, certainly in very varied conjunctions, even though the clinical picture may appear at first sight ever so divergent.
Consciousness is for the most part somewhat clouded, sometimes even very considerably, in catatonic morbid states, especially during their development and at the height of acute disorder. The patients appear, it is true, almost always to perceive single impressions fairly well, even when one cannot prove it at first, but still they usually have only a rather indistinct idea of their situation and of the occurrences in their surroundings, certainly partly on account of the fact that they are not at all concerned about them and do not feel the need to work up their perceptions further. They, therefore, often mistake people, do not know where they are, but cause surprise not infrequently by knowing the names of the nurses or of the other patients, by making a jocular remark, by complaining about some occurrence or other, by giving a reasonable account of their circumstances, by composing a connected letter with an accurate account of their place of abode and the request to be taken away.
Many patients also solve arithmetical exercises correctly, even of a somewhat difficult kind and display surprising knowledge; an apparently quite obtuse and inaccessible country lad could give accurate accounts of the Crusades and of Konradin of Hohenstaufen. Quite commonly discernment and clearness are much less disordered than one is inclined to assume from the singular demeanour of the patients which is essentially dependent on volitional disorders.
Insight
Even a certain insight into their diseased state is frequently present. The patients call their singular doings stupidity; they say that they are just mad. To the question whether he was mentally affected, a patient replied:
Yes, of course! If one is sensible, one does not do such things!
A female patient, who displayed catatonic stereotypies of movement in the highest degree, said to me:
But I must always make such stupid movements; it is really too silly
Another complained that she always had to make faces, her laughing should be driven away. Many lay stress upon the fact that when they laugh they do not feel at all merry. A satisfactory account of the motives for their singular behaviour is certainly never got from the patients. A patient gave as the motive of his mutism the answer:
I am not yet suitable to be able to show a voice
Another stated that he had given utterance to his thoughts only in writing because he could not at once find words; a third said he had not spoken because he knew no one. A female patient said that she had not wished to speak, another that she did not venture to speak. The physicians had already known everything, the questions had been so simple, they had not known what they should say, are similar utterances. On being asked the motive of her refusing to eat, a patient declared that she simply did not need to eat; another asserted that she had not been hungry. Usually one is told that the patients were obliged to do what they did:
was obliged to spit
said a patient. Another declared that she was obliged to speak so, it was given to her so; a third on being asked why she assumed such peculiar attitudes answered:
Because I wish to.
Similarly a patient declared that he had remained so motionless because he had wished it; another alleged that he had been obliged to behave in that way, he had been unconscious. It had just amused them, come into their head, they had thought it had to be so, a power, an impulse, a force had come over them, are answers that frequently recur. Automatic obedience is explained by the fact that it had just been wished so, that the patients had thought that they were doing the physician a pleasure.
Much more rarely are other motives alleged. A patient according to his own account had believed that he would apostatize from God if he ate; a female patient said that God had not wished it; another said that he had been drawn to his violent movements “as with a rope,” a third who in counting always left out the number four, said that he always had to think at the same time of the fourth commandment. A fourth who for hours played passionately on the mouth-harmonica, affirmed that the omnipotence of God inspired him to make music in order that the military should take no harm. It can be clearly enough recognized from all these alleged motives, that the singular actions are of impulsive origin and do not depend on definite deliberation.
In spite of these clear statements about the peculiarity of their condition which in general is usually regarded as diseased, the patients have, at first at least, no real understanding of the gravity of the disorder. Many patients complain bitterly about the treatment which has been accorded to them; an extremely stuporous patient who for a full year had sat huddled up in bed, whose sensitiveness to pin-pricks had been tested, and whom one had often tried to put in a lying position, was enraged after sudden awaking from the stupor because she had been thrown into bed and that iron bars had been bored into her head. Another demanded 30,000 marks damages. To all representations of the incomprehensibility and morbidity of their conduct the patients give as answer explanations which say nothing, they had just not known where they were, were without cause torn away from their domesticity, had been treated in quite the wrong way; it was then not to be wondered at, if they had become somewhat confused.
Recollection of the period of the disease appears as a rule to be fairly clear, but very imperfect. The patients state that it may well be possible that this or that has happened so, but they did not know about it, neither could they explain how they had behaved as they did. Sometimes they dispute some of the occurrences very resolutely; then again assert that they have been dead, have been overpowered. The intermingling of delusions and hallucinations on the one hand, the inaccessibility and lack of insight of the patients on the other hand, make it often difficult to obtain a reliable account of the real substance of their recollections. The indifference, however, with which the patients regard their own serious malady is almost always very striking. They do not feel any real need to explain to themselves the details of their morbid experiences, do not ask about the subject, will not listen to anything about it, smile incredulously when they are told about it, do not attribute any very grave import to the disorder; regard themselves at once as perfectly well, as soon as they have become to a certain degree clear and quiet, insist without more ado on discharge, blind to better counsel.
Mood
Mood in states of stupor usually shows no marked colouring. Often the patients appear to be in a state of anxious tension, so that formerly a section of these cases was named “melancholia attonita,” as the rigidity was connected with emotions of anxiety and fearfulness. It is as a rule easy to convince oneself that fear is not the motive of the patients’ behaviour. They are not influenced by threats, do not draw back from the clenched fist or the drawn knife, do not blink when the point of a needle is brought near their eye. Only in the beginning of the disease do we occasionally notice, corresponding to the depressive delusions, outbreaks of violent fear and despair. Later the mood changes often without recognizable cause; pitiful weeping gives place to furious irritation or childish merriment, while a dull indifference forms the basis, and is expressed particularly in the behaviour of the patients to their nearest relatives and in the gradual disappearance of wish and will.
The General Course
The general course of the catatonic forms is very varied as already appears from the description given. It shapes itself in still more changing forms because in about one-third of the cases considerable improvement in all morbid phenomena, sometimes resembling complete recovery or coming very near it, occurs, most frequently as it seems in the cases beginning with a state of depression. The duration of these periods of improvement varies greatly; they most frequently last about two to three years; but they sometimes last nine, ten, twelve, thirteen, fourteen, sixteen years; indeed once between the first attack of the disease and the second which led to dementia, there was an interval of twenty-nine years. The objection can certainly always be made, that in the case of such long intervals the two attacks have nothing at all to do with each other. Meanwhile the observation that a pause of ten years’ duration between two attacks with quite similar morbid phenomena is frequent in this as in other forms of dementia praecox, shows there cannot well be any doubt here about a long respite and renewed outbreak of the same morbid process. But then also we often enough see the insidious development of the malady extended over long, long years till at last an acute disorder announces the real outbreak of the disease. Not altogether seldom the disease runs its course in three, or still more, attacks separated by periods of improvement, attacks which in certain circumstances may at first be of only quite short duration before a more serious one commences leading to dementia. The individual catatonic states may either follow the one immediately after the other and alternate quickly, or be separated from each other by long intervals. I observed a case where a state of excitement followed the introductory stupor only after fifteen years; in other cases the malady began with a state of stupor which was first interrupted by a remission of many years and then a characteristic state of excitement developed. In another case stupor appeared only after the malady had lasted for fifteen years.
In the terminal states dementia along with the phenomena of negativism and mannerisms was in great excess. Simple weak-mindedness was the issue in about 11 per cent. of the cases, dull dementia still somewhat more rarely. Seizures were observed in 17 per cent. of the cases. A female patient, thirty-one years of age, broke down completely a few days after an attack with deep unconsciousness and unilateral manifestations of cerebral irritation. On the whole we must reckon the catatonic forms with the more unfavourable varieties of dementia praecox on account of the frequency of profound dementia, while passing improvements are somewhat more frequent than in the average of the cases here taken into account. The share of the men with 54 per cent. and of the cases under the age of twenty-five with 57 per cent. does not deviate from the average; still the forms beginning with stupor seem to me to begin at a somewhat more advanced age. The number of the observed cases included 19.5 per cent. of the whole series.
The Paranoid Dementias
A picture, which is in many respects divergent, is exhibited by those cases, the essential morbid symptoms of which are delusions and hallucinations; we call them paranoid forms. I feel justified in including them in the domain of dementia praecox by the circumstance that in them, sooner or later, a series of disorders of a kind which we everywhere find also in the other forms of dementia praecox, invariably accompanies the delusions. Further in a large number of cases terminal states are developed, which completely resemble the forms described up to now, and also in the remaining cases a psychic decline is developed, which in spite of many peculiar features, nevertheless discloses a near relationship with the issues of dementia praecox already known to us.
Paranoid Dementia Gravis
If, as seems conformable to our purpose, we let ourselves be guided in the grouping in detail by the point of view of prognosis, we shall next have to take into consideration those paranoid morbid states, which, it is true, begin with simple delusions, in the further course, however, exhibit always more distinctly the peculiar disintegration of the psychic life, and in especial also the emotional and volitional disorders in the form characteristic of dementia praecox; they might be grouped together under the name of “dementia paranoides gravis.”
The development of the disease took place in 68 per cent. of my cases insidiously; in 17 per cent. of the patients there